Hearing abilities vary from person to person, so it is important to assess hearing to identify individuals with hearing loss. Different methods of hearing testing are used for this purpose. These methods can be formal or informal. Some tests only help to detect the presence of hearing loss, while others provide detailed information about which part of the ear is affected and help in deciding the appropriate treatment or rehabilitation. Therefore, hearing testing plays a crucial role in the early identification and management of hearing loss.
Hearing Testing
Hearing tests help in understanding the actual hearing ability of an individual. Through these tests, we can identify the type and degree of hearing loss, which is important for proper diagnosis. Some hearing tests also provide information about how well a person can perceive and understand speech. This helps in planning suitable treatment and rehabilitation for the individual.
Methods of testing hearing
There are several methods available for testing hearing, which are broadly classified into screening tests and diagnostic tests. Screening tests help to identify whether an individual has a hearing loss or not, but they do not provide details about the type or degree of hearing loss. Diagnostic tests, on the other hand, are conducted by an audiologist to determine the extent and nature of the hearing problem.
Hearing tests can also be categorized as behavioural (subjective) and physiological (objective) tests. Behavioural tests require an intentional response from the individual to sound, while physiological tests do not require any response and measure the body’s automatic reactions to sound.
An audiologist usually uses a combination of tests, depending on factors such as the individual’s age, symptoms, associated conditions, and purpose of assessment. Based on the results, the audiologist diagnoses the problem and refers the individual for appropriate management. If the issue lies in the external or middle ear, the person is referred to an ENT specialist. In cases of sensorineural hearing loss, hearing aids may be recommended after medical clearance. If a problem in the auditory nerve or nervous system is suspected, the individual is referred to a neurologist.
- Tuning fork tests
- Pure-tone audiometry
- Speech audiometry
- Immittance evaluation
- Auditory brainstem response (ABR/BERA)
- Otoacoustic emissions
Before administering any of these tests, a detailed case history has to be taken to record the complaints of the client.
Tuning fork
Tuning fork tests are simple and quick methods used to get a basic idea about the type of hearing loss in an individual. A 512 Hz tuning fork is commonly used, which is made to vibrate by striking it against the elbow or knee.
Two commonly used tuning fork tests are the Rinne test and the Weber test. In the Rinne test, the vibrating tuning fork is first held near the external auditory meatus to check air conduction. Then, it is placed against the skull behind the ear (mastoid area) to check bone conduction. The individual is asked to compare which sound is louder.
The comparison between air conduction and bone conduction helps in identifying the type of hearing loss, as the responses vary depending on whether the hearing loss is conductive or sensorineural.
- In individuals with normal hearing the tone will be more audible near the external ear.
- In individuals with sensorineural hearing loss the tone is audible at the external ear. Tis is called Rinne-positive.
- In individuals with conductive hearing loss the tone is audible through bone conduction. This is called Rinne-negative.
The weber’s test was developed to detect unilateral hearing loss. It compares bone conduction in both ears. A vibrating 512Hz tuning fork is placed on the center of the patient’s forehead. The patient is asked whether the sound is heard in the middle or to one side.
- If the sound is louder on the side in which the hearing loss is present then the person may have a conductive hearing loss.
- If the sound is not louder on the side in which the hearing loss is present then the person may have a sensorineural hearing loss.
Other lesser known tuning fork tests are:
- Bing test
- Schwabach test
We should remember that tuning fork tests are not usually recommended to be used as they give unreliable results. It is always better to use an audiometer to check a person’s hearing ability.
Audiometry and parts of an audiometer
An audiometer is the most basic instrument used for testing hearing, available in both portable and desk types. It is classified based on the facilities it provides, with the minimum function being pure-tone testing through air conduction. Most audiometers also include bone conduction testing.
For air conduction testing, sound is delivered through headphones or insert earphones, while for bone conduction testing, a bone vibrator is placed on the mastoid bone behind the ear. Advanced audiometers may also include features like speech audiometry, masking, and special tests such as Tone Decay Test (TDT), Alternate Binaural Loudness Balance (ABLB), and Short Increment Sensitivity Index (SISI), which help in detailed hearing evaluation.
Audiometers usually operate on electric power (AC), although some screening audiometers may use batteries. A pure-tone audiometer produces a pure tone (single frequency sound), and both its frequency and intensity can be adjusted.
For air conduction testing, frequencies typically range from 250 Hz to 8000 Hz, while for bone conduction testing, they range from 250 Hz to 4000 Hz. The intensity range for air conduction is generally from -10 dB HL to 120 dB HL, whereas for bone conduction, it is lower and usually does not exceed 50–70 dB HL depending on frequency.
Thus, an audiometer is an essential tool for accurately assessing hearing ability and identifying hearing loss.
Some of the basic controls available in an audiometer are as follows:
- A frequency dial to vary the frequency of the signal generated.
- An intensity dial to vary the intensity of the signal generated.
- An interrupter switch to present the signal
- An output selector for selection of transducer (supra aural earphones, insert earphones, loud speakers or bone vibrator) and ear to be tested.
Audiogram
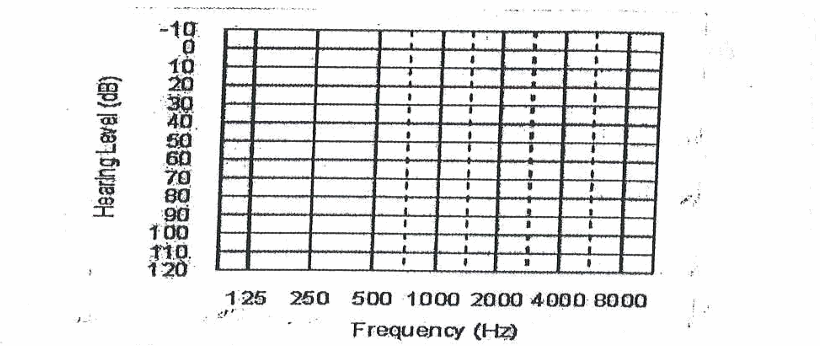
The results of hearing tests are represented on a graph called an audiogram, which shows a person’s hearing ability. In an audiogram, frequency (pitch) is plotted on the horizontal (X-axis) and measured in Hertz (Hz), while intensity (loudness) is plotted on the vertical (Y-axis) and measured in decibels (dB HL).
Frequencies start from low on the left side (125–250 Hz) and increase to high on the right side (up to 8000 Hz). The intensity scale ranges from soft sounds at the top (-10 or 0 dB HL) to loud sounds at the bottom (around 110 dB HL). It is important to note that 0 dB HL does not mean absence of sound, but rather the softest sound that a normal hearing person can detect.
Different symbols are used to represent results:
- O → Right ear (Air Conduction)
- X → Left ear (Air Conduction)
- < → Right ear (Bone Conduction)
- > → Left ear (Bone Conduction)
Usually, the right ear is marked in red and the left ear in blue. The results can be plotted either on separate graphs or on a single audiogram for both ears.
Pure Tone audiometry
Case History
The first step in hearing assessment is obtaining a detailed case history. This involves interviewing the client and/or their informant to gather important information about the nature of the hearing problem and any associated conditions.
A proper case history helps in understanding the individual’s difficulties, identifying possible causes, and planning suitable tests and management. It usually includes details related to the onset of hearing loss, medical history, family history, communication difficulties, and other associated problems.
- Demographic information such as name, age and gender of the client.
- Education and occupation.
- Age of onset of hearing problem.
- Whether the problem is in one ear or both ears.
- Whether the problem started suddenly or gradually.
- Whether the problem is increasing day by day.
- Whether the client has a complaint of: a) Ear Pain
- History of any illness or injury that could be associated with hearing loss, medication taken for illness.
- Whether the client is/was exposed to loud sounds.
- In case of children, any illness/injury that could lead to hearing loss when the mother was pregnant or during the birth of the child (prenatal and natal history)
- Associated problems.
- Family history of hearing problem.
- Reports of previous evaluation and treatment.
Information collected from case history is helpful for the tester to decide the type and procedure of tests that needs to be carried out for the client. Case history also gives valuable information while diagnosing and making appropriate referrals for the client.
Procedure for pure tone audiometry
Pure-tone audiometry should be conducted in a noise-free environment, as even soft background sounds can affect test results. Therefore, testing rooms are acoustically treated according to national and international standards to minimize noise. Ideally, audiometry is performed in a two-room set-up, where the audiologist and the patient are in separate rooms. If this is not available, a single-room set-up may be used.

This test assesses the hearing ability of each ear separately at different frequencies. It helps determine the hearing threshold, which is the lowest intensity of sound a person can hear at least 50% of the time.
Pure-tone audiometry includes both air conduction and bone conduction testing. For air conduction, sounds are presented through headphones, insert earphones, or loudspeakers, while for bone conduction, a bone vibrator is placed on the mastoid bone. This method helps in identifying the type and degree of hearing loss accurately.
The procedure for obtaining pure-tone thresholds includes the following steps:
- Seat the client or the subject on a comfortable chair.
- Take a detailed case history to get information regarding this present and past complaints related to hearing.
- Examine the client’s ear to ensure that the ear canal is free from wax, foreign body or debris. If not, refer the client to an ENT doctor.
- Give the following instruction to the client: ” A sound will be presented to your ears. If you hear a sound, raise your finger/hand. When you stop hearing the sound put down your finger/hand. The loudness of the sound may vary. Even if you hear a soft sound, raise your finger/hand”.
- If a client is a young child who cannot follow instructions or the client does not have sufficient speech and language to follow instructions, play audiometry is carried out. In play audiometry, blocks, marbles or any item which the child likes are used for training the child. The child is trained to carry out a play activity such as putting down a block or rolling a marble every time he/she hears a sound. If a child cannot be trained for play audiometry and other physiological tests such as auditory brainstem responses, otoacoutic emissions are carried out.
Air conduction testing
- Place earphones over the ears. Note that the headset generally has a blue mark on one earphone and a red mark on the other. Place the headset in such a way that the blue earphone is placed over the left ear and the red earphone is placed over the right ear.
- First test the better ear (as reported by the client). If you do not know which the better ear is, test the right ear first.
- Choose 1000 Hz on the frequency dial and 40 dB HL on the intensity dial. Press the interrupter to present the signal.
- Repeat this procedure until you find out the lowest intensity that can be heard by the client. The lowest intensity at which the client responds at least 50% of the time is plotted as his/her threshold at that frequency.
- Change the frequency to 2000 Hz and repeat this procedure.
- Repeat the procedure to obtain threshold at 4000 Hz and and 8000 Hz.
- Repeat threshold at 1000 Hz. Then obtain threshold at 500 Hz and 250 Hz.
- Repeat the entire procedure to obtain thresholds for the other ear at 1000 Hz, 2000 Hz, 4000Hz, 8000Hz, 500 Hz and 250 Hz.
Bone Conduction Testing
- Place the bone vibrator on mastoid bone behind the pinna. Bone vibrator is generally placed on the mastoid of the better ear and the thresholds obtained are called as common bone conduction threshold. If air conduction thresholds of both the ears are similar, then place the vibrator on the right ear.
- Obtain bone conduction thresholds from 250 Hz to 4000 Hz using the same steps used for air conduction testing.
Different types of audiograms
A hearing loss is described in terms of the type, degree and configuration of the audiogram. The following information plotted in an audiogram is used for explaining the type, degree and configuration of hearing loss:
- The average amount of hearing loss by air conduction and the amount of hearing loss by air conduction at different frequencies.
- The amount of hearing loss by bone conduction and the difference between air conduction threshold and bone conduction thresholds.
Type of hearing loss:
The difference between air conduction and bone conduction thresholds, the air-bone gap, gives information about type of hearing loss. Following guidelines are used to classify the hearing loss into different types.
Conductive hearing loss: An individual is said to have conductive hearing loss if his/her bone conduction thresholds are normal but air conduction thresholds are affected.
Sensorineural hearing loss: An individual is said to have sensori-neural hearing loss if both air and bone conduction thresholds are affected to the same extent. That means hearing thresholds for both air and bone conduction are abnormal and the air-bone gap is less than 10 dB.
Mixed hearing loss: An individual is said to have mixed hearing loss if both air and bone conduction thresholds are affected but the amount of loss by air conduction is more than that by bone conduction. That means the air bone gap is more than 10 dB in individuals with mixed hearing loss.
Degree of hearing loss:
Amount of hearing loss by air conduction is used to describe the degree of hearing loss. Hearing loss is classified into different degree based on pure-tone average for air conduction thresholds. The pure-tone average (PTA) refers to the average of air conduction thresholds at 500 Hz, 1000 Hz and 2000 Hz. One of the commonly used classifications of degree of hearing loss is that given by clark (1981). The guidelines for the classification given by clark (1981) are as follows;
| PTA Less than 15 dB HL | Normal hearing |
| PTA of 16 to 25 dB HL | Minimal hearing loss |
| PTA of 26 to 40 dB HL | Mild hearing loss |
| PTA of 41 to 55 dB HL | Moderate hearing loss |
| PTA of 56 to 70 dB HL | Moderately severe hearing loss |
| PTA of 71 to 90 dB HL | Severe hearing loss |
| PTA >90 dB HL | Profound hearing loss |
Configuration of hearing loss
The shape or configuration of an audiogram depends on the amount of hearing at different frequencies. Hearing thresholds are usually not the same across all frequencies, which results in different patterns on the audiogram.
If hearing loss mainly affects the high frequencies, it is called a high-frequency hearing loss. In this case, hearing is better for low frequencies and poorer for high frequencies, resulting in a sloping configuration.
If the hearing loss affects the low frequencies, the audiogram shows poorer hearing for low tones and better hearing for high tones. This pattern is known as a rising configuration.
In some cases, the hearing loss is equal across all frequencies, and this is called a flat configuration.
Thus, the configuration of an audiogram helps in understanding the pattern and nature of hearing loss.
Bilateral versus unilateral:
Bilateral hearing loss means both ears are affected. Unilateral hearing loss means only one ear is affected.
Symmetrical versus asymmetrical:
Symmetrical hearing loss means that the degree and configuration of hearing loss are similar in both the ears. An asymmetrical hearing loss is one in which the degree and/or configuration of the loss is different for each ear. In client with unilateral or asymmetrical hearing loss, special procedure called masking is required during pure-tone audiometry. Masking is used to prevent the participation of better ear while testing the poorer ear.
Factors that affecting hearing testing
A number of factors related to the subject/client, test environment, instrument and test procedure used for testing could affect the results of pure-tone audiometry. Some of the factors that can affect the test results are listed here:
- Client’s ability to understand instructions for the test
- Co-operation of the client.
- Motivation of the client
- Attention of the client
- Noise levels in the test room
- Reverberation (Reverberation refers to the amount of signal that is reflected from the walls of the room) and temperature inside the test room.
- Calibration of the instrument (Calibration checks whether the signals presented through the instrument are same as what it is supposed to be)
- Procedure used for testing.
Speech Audiometry
Speech audiometry is used to assess a person’s ability to understand speech, which reflects everyday listening more accurately than pure tones. It provides a clearer idea of an individual’s functional hearing ability and helps in predicting the benefit from hearing aids.
Speech audiometry is conducted using an audiometer and includes three main tests: Speech Detection Threshold (SDT), which measures the ability to detect speech; Speech Recognition Threshold (SRT), which determines the lowest level at which speech can be understood; and Speech Identification Scores (SIS), which assess how well a person can correctly recognize and repeat words.




